Here’s an article from the American Psychiatric Association, intended to introduce the new diagnosis of Prolonged Grief Disorder. It’s scheduled for inclusion in the DSM as of March of 2022.
APA Offers Tips for Understanding Prolonged Grief Disorder
I’ve long been fascinated by cases where seemingly “normal” grief persists for many months or even years. The new disorder recognizes this phenomenon and provides a framework for identifying and evaluating such cases.
In truth, prolonged grief has been around for as long as I can recall. It’s in focus now as the world confronts the awful death toll associated with the coronavirus pandemic. In the US alone, best estimates are between six and eight hundred thousand fatalities, to date. That’s probably an undercounting, by the way, akin to what we suspect happened during the current opioid epidemic. The number of actual drug-related deaths probably greatly exceeds the estimated 700,000.
As for the human cost of COVID: one pro basketball star reports having lost seven family members to the disease. What is a ‘normal’ grief process for someone who experiences that degree of loss in a relatively short period? I’m glad to know that scientists are busy studying the phenomenon, perhaps coming up with ways to address the damage done.
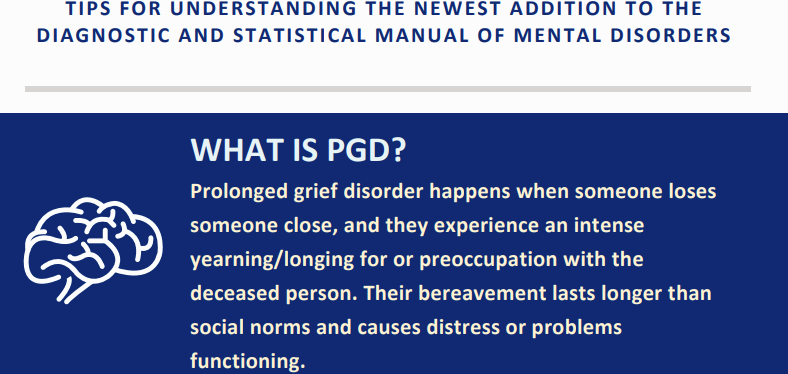
With adults, the disorder is usually found within 12 months of a death. I expect there will be exceptions. The article contains a link to an Infographic that clinicians can copy or print for quick reference.
In general, the pathology of prolonged grief centers around intense feelings of longing for the deceased, or preoccupation with thoughts of him or her, reported on most days or even daily. Symptoms produce clinically significant distress or cause impairment in key functions. There’s the usual qualification that the syndrome isn’t better explained by another mental health disorder. And allowances to make for the different ways societies, cultures, and religions deal with death and dying.
That’s an issue that comes up frequently here in New Mexico, where Hispanic and Native cultures have their own strong beliefs and traditions. They were well-established here in the Southwest, long before the United States came into existence.
The APA offers the following list of symptoms for use by clinicians:
- Identity disruption (e.g., feeling as though part of oneself has died).
- Marked sense of disbelief about the death.
- Avoidance of reminders that the person is dead.
- Intense emotional pain (e.g., anger, bitterness, sorrow) related to the death.
- Difficulty moving on with life (e.g., problems engaging with friends, pursuing interests, planning for the future).
- Emotional numbness.
- Feeling that life is meaningless.
- Intense loneliness (i.e., feeling alone or detached from others).
I imagine most if not all working clinicians have encountered such a case. It’s sometimes shunted to one side under a heading like ‘persistent depression’. That’s not ideal, since this represents a singular type of mood disorder that may not respond as hoped to conventional therapies.
One case from many years ago: a woman was entrusted with care of her infant grandchild while the child’s parents went out for dinner. She just wanted to give the young parents a break. But once they left, she decided to open a bottle of wine and have a glass while she watched an evening’s TV.
A few hours later, the parents returned to find grandmother passed out on the couch. Their child, tragically, had stopped breathing long before.
I can only imagine what that’s like. Still, I understand that eventually, with considerable help, she succeeded in recovery.
Anyway, despite all the attention paid to grief and how to cope with it, there remain a host of unanswered questions, especially about grieving that lasts, and lasts, and lasts.
Let’s hope the additional attention helps us address some of those gaps in understanding.







{kind=link}