This crossed my inbox recently, from Medscape: findings from a research study on the impact of Transcranial Magnetic Stimulation (TMS) for AUD patients. Here’s a link, but I’ll describe the findings as well, just in case:
Transcranial Magnetic Stimulation Shows Promise for Alcohol Addiction
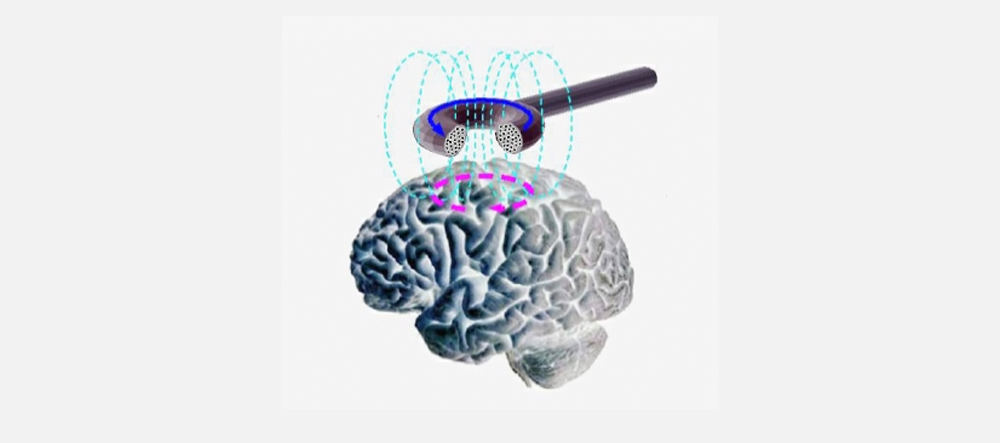
If you aren’t familiar with TMS, we’ll include something from the Mayo Clinic on its use to treat depression.
I first heard of TMS when a local neurologist began promoting it– for smoking cessation. Had to be in the late 1970s or early 80s. A couple of our former detox patients, heavy smokers in early recovery, signed up. I think they subsequently dropped out. Those were early days, and the practice is no doubt much refined since then.
According to the article, “In a randomized, double-blind, sham-controlled trial, participants who received TMS… for 3 weeks showed significantly reduced heavy drinking days compared with a group who received a sham treatment.”
A sham treatment, if you’re unfamiliar with the term, is akin to a placebo in a medication trial. The sham is something that has already been shown to have no impact on the target behavior.
Subjects received TMS treatments in 30-minute increments during the week. The principal impact on alcohol use turned out to be with respect to the number of days where ‘heavy drinking’ occurred. Heavy drinking is defined here as a minimum of five drinks containing 12 grams of pure alcohol daily for men, or four drinks for women.
According to NIAAA, a standard drink in the US contains roughly 14 grams of pure alcohol. That could be found, for instance, in 12 ounces of 5% beer, 5 ounces of 12% wine, or 1.5 ounces of 40% distilled spirits.
Drinking 60 grams of pure alcohol a day for a week would represent, I’m told, around 20 pints of beer. Sounds like a lot, and it is.
“Not for me it isn’t,” admitted a clinic patient.
I don’t know if TMS will ever prove to be widely useful in treatment for AUD, or become a ‘niche’ product for specialty use. It all depends on how well it translates from the research setting to the world of clinical practice, in terms of affordability, practicality, and patient acceptance. BTW, these are only Stage 1 findings, so Stages 2 and 3 of the research are yet to come. We’ll have to see how the results hold up.
For me, it was encouraging to see how far science has come in its understanding of the neurological underpinnings of alcoholism. That was pretty controversial in the days when alcoholism was still primarily considered a psychological disorder. Simply to assert that neurophysiology played a primary role in its origins was viewed as quite radical.
I’m glad to see that changing.











{kind=link}