It’s not that easy to predict how Cannabis Use Disorder (CUD) will affect addiction treatment going forward. There are a number of factors involved.
First, the sheer scale of the problem. I’ve come across reports that claim some 18 million Americans qualify for a CUD diagnosis. That sounds like a lot until you realize exactly how many Americans have used cannabis. It’s second only to alcohol.
I found that easy to believe, given the trend towards legalization and the wild growth of a commercial cannabis industry. Not that the black market has suffered. It’s still going strong.
So it seems to me that since we’ve made it easier to buy and use pot (and pot products) than ever before, we can expect continued rapid growth in the foreseeable future. Industry investors certainly seem confident.
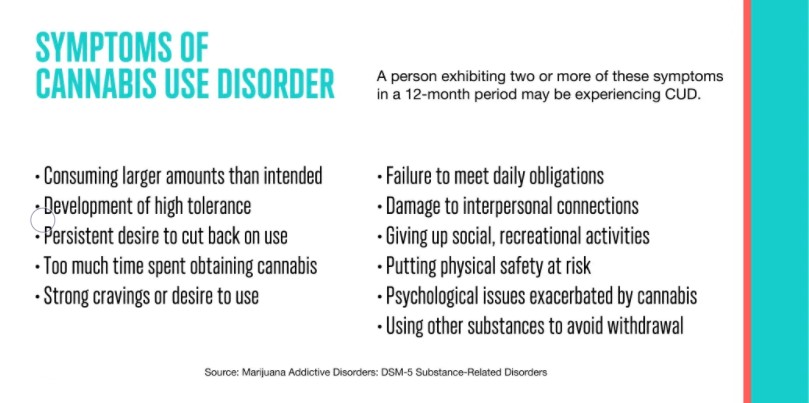
Research tells us that the bulk of CUD cases, especially among newer users, will fall into the ‘mild’ category — meaning they’ll meet two or possibly three criteria out of the eleven listed in DSM5. Not enough to motivate a typical user to seek help.
No, it’s likely to be those with five or six or more symptoms — the high-moderate to severe cases — that eventually seek treatment. Some of those will be ‘poly-drug’ users, with multiple problems involving multiple drugs.
It’s not uncommon for someone to present for treatment of an opioid, alcohol, or stimulant problem, while also having a significant problem with cannabis that they may not even recognize. Perhaps they were preoccupied with other, ‘harder’ drugs.
That’s not good, because a moderate/ severe CUD often means experiencing cannabis withdrawal symptoms, as well as intense cravings for the drug, and repeated (failed) attempts to stop using it. These symptoms can easily undermine early efforts to recover from opioid, stimulant, and alcohol disorders.
And open the door to a return to other drug use, perhaps of a far more dangerous kind.
That’s why whenever CUD is present, we should take the time to identify and treat it, along with the other SUDs.












{kind=link}