Let me start with a clarification: Needle exchange was never intended to be an ‘anti-opioid’ approach. It’s certainly not treatment, and the goal isn’t to eliminate or even significantly reduce someone’s opioid use. I guess whoever wrote the heading for this article wasn’t aware of that.
Republicans rebel against a powerful anti-opioid tool
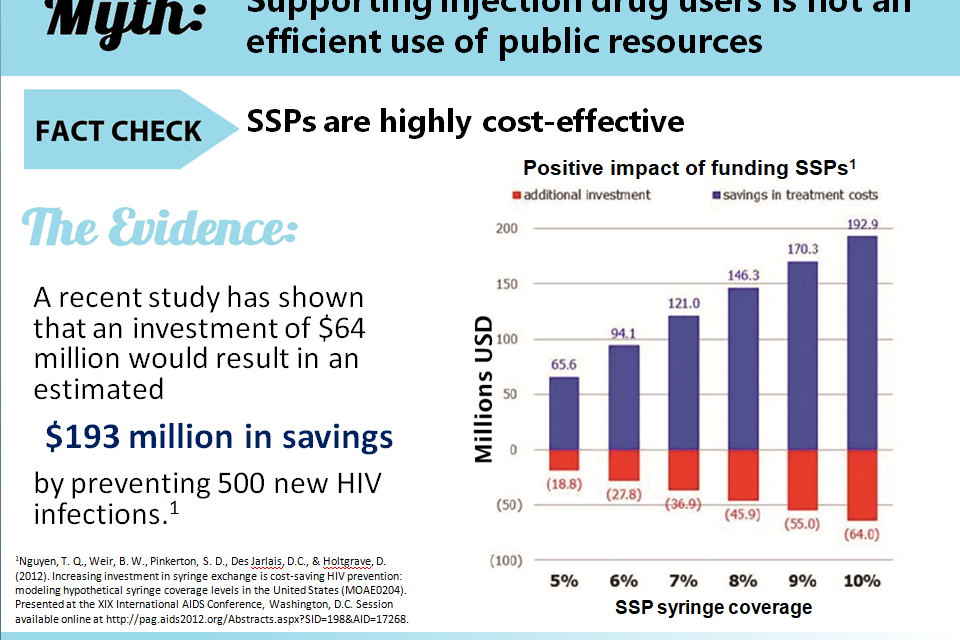
Needle exchange was one of many programs implemented in response to HIV/AIDS — a disease which arose without warning and has killed more than 700,000 Americans. Along with unprotected sex, a major avenue for the spread of HIV was the common practice of sharing used or ‘dirty’ needles. By offering to exchange those dirty needles for clean ones, public health officials hoped to reduce transmission from one needle user to another. That also helped prevent further spread of hepatitis B and C, two more blood borne diseases.
By all reports, it seems to have worked. Not perfectly, of course, but with measurable positive outcomes.
Just as it isn’t there to lead users to stop using drugs, neither does it encourage others to begin. A certain percent of those who participate in needle exchange will eventually enroll in addiction treatment. But that’s to be viewed as a welcome side benefit, not the primary reason for the program’s existence.
From a public health perspective, it’s simply one practical solution to a very challenging problem. Still, the public has often treated it with suspicion. Some because they feared it would encourage local kids to experiment with drugs — we’ve covered that already — or worse yet, attract criminals and criminal activity to the area. I recall attending one meeting where a local man stood up to berate health officials for threatening the good name of his neighborhood. He insisted that people would hear about the existence of a needle exchange program in the vicinity and conclude that this must be a ‘bad part of town’. Which, he claimed, would drive down property values.
As soon as he was finished, someone else stood up to protest that as far as she could tell, their neighborhood already had a bad reputation for drug use, and programs like this might improve things. But why, argued a third speaker, can’t it be located somewhere else? Why here?
That’s a familiar argument whenever recovery homes or treatment clinics seek to locate close to residential areas. Even has its own acronym: NIMBY.
In some cities, a compromise was reached. Needle exchange could be offered during limited hours on scheduled days, via health department vans parked in church lots. At least that way they were less visible.
Things did quiet down, and the programs got under way. But now, spurred on by pandemic anxiety, resistance has again crystallized in the form of renewed efforts to shut down or block needle exchange programs. Even in some areas where they seem well-established.
Let’s just hope the opposition doesn’t succeed. We don’t need another AIDS outbreak on top of COVID-19.
It helps to remember that this kind of resistance to a public health initiative of proven value is based in fear, and that level of feeling doesn’t readily respond to scientific argument. In the heat of the moment, we worry that the public will be persuaded to take actions that are ultimately not in their own best interests.
That happens quite often. During the pandemic, it’s actually on the rise. There will be a price to pay later, no doubt in terms of illness and death. There always is.










{kind=link}