This is actually the third time we’ve looked at the mega-popularity of gabapentin, brand name Neurontin, in the context of possible misuse.
The first instance involved a number of clients from one large methadone program who visited the same local physician for different reasons, yet all managed to leave with a prescription for gabapentin. The second concerned a surge in the number of young adults who arrived at a family clinic clutching an expired prescription for unusually high doses of the medication. They were seeking a new order at the same elevated dosage.
Now comes an article in The New York Times addressing the problem in terms of off-label prescribing to an especially vulnerable population: senior citizens.
Seniors are known for visiting the doctor’s office more often than other people, for a wider range of problems. Gabapentin seems to have become a kind of “default” remedy for their complaints — “the drug you prescribe,” a physician told me, “when you don’t have anything of real value to offer.”
A script for gabapentin, he implied, can mean a patient who leaves the office at least somewhat satisfied with services received. Makes for a better rating on the post-visit comment card.
“Don’t forget,” one physician reminded me. “gabapentin isn’t a controlled substance in my state.” Not yet, at least. Meaning no need to worry about getting in trouble with the authorities for having prescribed too much of it.
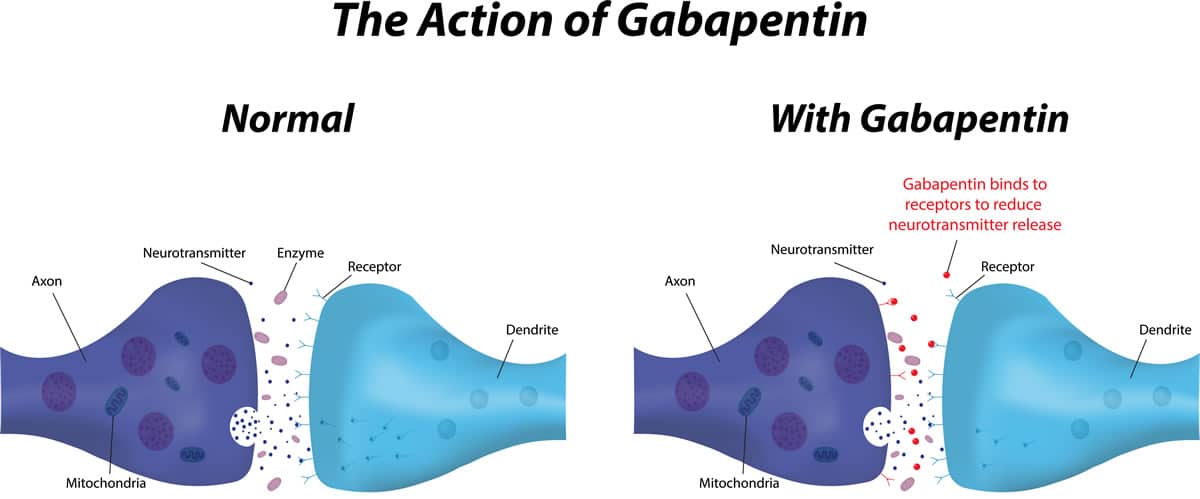
It isn’t difficult to understand why gabapentin became so popular, as a less risky alternative to prescribing opioids for chronic pain during an opioid epidemic.
Is it actually effective for treating pain, however? Research suggests not very. The evidence in favor is scant.
“The history of gabapentin is really a history of uses getting ahead of the evidence,” according to an expert quoted in the Times. That includes a willingness to ignore the drug’s side effects, including oversedation and dizziness — always an issue with seniors, who are prone to falling, sometimes with extremely serious consequences.
So why do physicians keep prescribing gabapentin?
My guess would be it’s because they feel they don’t yet have a better alternative.
After all, patients still show up wanting something for whatever ails them. It isn’t easy for a physician to ‘just say no’ — even if that’s the approach the evidence supports. It’s still more difficult in the context of an 8 to 12 minute physician visit.
With so many scripts being written for Medicare recipients, I imagine the government will have to step in at some point. Probably with some level of regulation.
How much regulation, or what kind, remains unknown.











{kind=link}