I first became aware of the risks associated with gabapentin (AKA Neurontin) back in 2017. Following some further investigation, I became even more concerned. I expressed that in this post from January 2018.
After that, I’m afraid gabapentin dropped off my radar screen. Until a few days ago, that is, when I learned that Public Citizen, the prominent consumer advocacy organization founded by Ralph Nader, had formally requested of both the Food and Drug Administration (FDA) and the Centers for Disease Control (CDC) that steps be taken to classify gabapentin as a controlled substance, under Schedule 5. Then it would be subject to the same restrictions as common drugs such as Lomotil, Robitussin, and Lyrica.
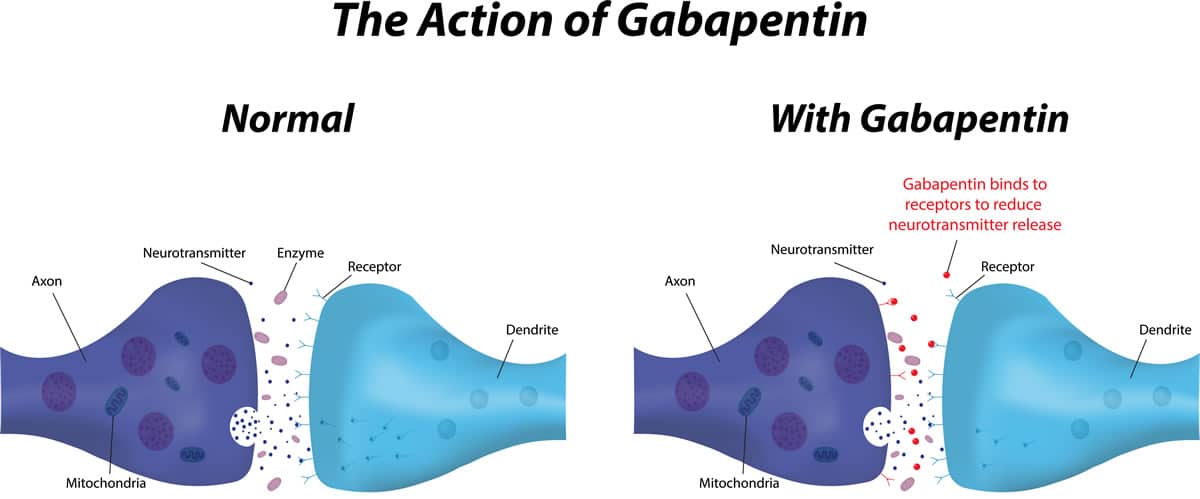
That’s important in terms of abuse because gabapentin has become very popular – last I looked, it was among the top twenty most prescribed medications in the US. It’s approved by the FDA for use in the treatment of epilepsy, post-shingles nerve pain, and Restless Legs Syndrome (RLS), but in practice? It’s far more widely prescribed. Easy to get, even.
I saw one estimate that 90% of prescriptions written for gabapentin were intended to treat problems such as chronic cough, hiccups, post-op pain, and menopausal hot flashes, among others. Those would have to be ‘off-label’ uses — prescribed by the physician outside of FDA approval.
As gabapentin use became more widespread, problems began to emerge. I heard complaints from clinicians on opposite sides of the country. One Pennsylvania clinical supervisor was concerned that many of this methadone clients were visiting local physicians specifically to obtain prescriptions for (you guessed it) gabapentin. This he believed was based less on genuine need than on word of mouth among methadone clients about how easy gabapentin was to obtain. Then I heard from a family physician in New Mexico that several new patients, all young, had come to the clinic claiming to be on unusually high doses of the drug, and in need of a new prescription.
Those are traditionally red flags for potential abuse. I wondered how many of those prescriptions would find their way onto the street, for sale or trade. As we’ve discussed before, any such medication in its original packaging is likely to bring a premium price, in dollars or drugs.
I asked around among my physician friends and wasn’t surprised to learn that many of today’s medical practitioners regard gabapentin as essentially harmless — on the grounds that it isn’t a controlled substance. They have few compunctions about writing gabapentin scripts because they don’t see it as a potential risk. That’s based mostly on its legal status. “Where the downside?” one told me. “You can’t really abuse the stuff.”
Oh yeah? In some circles, it’s already touted for its potential as an intoxicant. One website mentioned the drug’s popularity when the users mixes with other substances, such buprenorphine (Suboxone) and prescription opioids. I’ve also seen it promoted for use with cocaine, methamphetamine, and even caffeine pills.
I know — what’ll they think of next? Something, I’m sure.
Once again, we have an opportunity to recognize a problem before it’s widespread and take steps to prevent it. Let’s hope we do just that.











{kind=link}