When I first began working in addiction treatment, the term Detox Program was ordinarily used to describe one of two options. They were:
- A 3 to 5 day stay in a hospital, probably with minimal attention from busy nurses, or
- A comparable stay in a freestanding social setting detoxification facility, where medication was not available, but there was plenty of support from the staff.
Both had their strengths and weaknesses. The hospital gave good medical care, but was prone to the revolving door syndrome: someone would be admitted late, heavily intoxicated, usually via the emergency room. They’d sleep through the night, only to “wake up, sit up, and throw up” prior to leaving against advice the following morning.
As you can imagine, this was not popular with the hospital or its staff. Especially since the same person would sometimes show up the following week for a return performance.
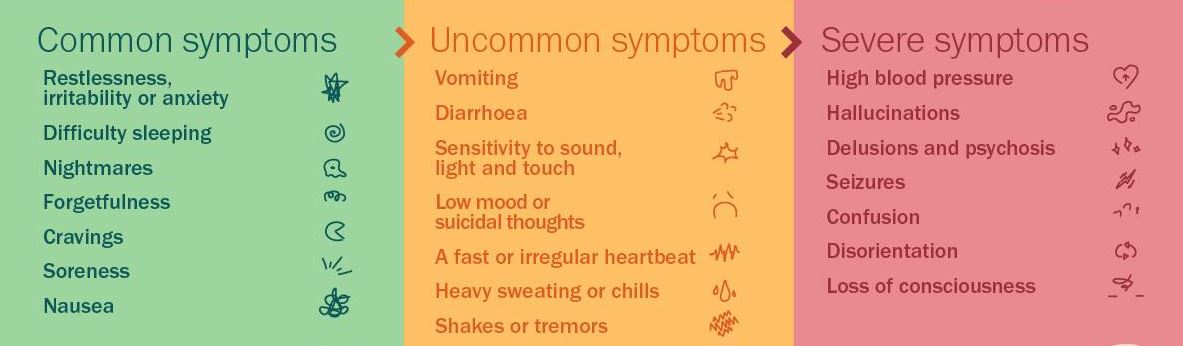
The social setting often provided a more supportive atmosphere for the detoxing patient, but since no meds were given, those they served were vulnerable to extreme discomfort, and sometimes seizures.
Amazingly, despite numerous failures, many of the patients who went through programs just like these nevertheless did quite well in recovery afterwards. I’m not sure if that was because of, or perhaps in spite of, the help they received.
We’ve come a long way since.
Now, detox has matured into withdrawal management, and the cookie-cutter approach is no more. It’s been replaced by a set of evidence-based practices, individualized through assessment to patient need.
The American Society of Addiction Medicine describes the various levels at which this may occur.
Level 1-WM (Ambulatory Detox without Extended On-site Monitoring): As you might imagine, this level is aimed at those with relatively mild withdrawal symptoms, few if any complicating conditions, and a supportive home environment.
Level 2-WM (Ambulatory Detox with Extended On-site Monitoring): Also an outpatient service, but enhanced by several hours of daily supervision from nursing staff. Here we should expect to find patients with moderate withdrawal symptoms and/or a less supportive home environment.
Level 3.2-WM (Clinically Managed Residential Withdrawal Management): Still no round-the-clock nursing care, but plenty of support and guidance from counselors and peers. This is a preferred solution for the many SUD patients who lack the internal motivation or the support at home to achieve their treatment goals.
Level 3.7-WM (Medically Monitored Inpatient Withdrawal Management): also a residential setting, but with 24-hour nursing and physician availability — intended to accommodate patients with moderate to severe withdrawal or other medical complications.
Level 4-WM (Medically Managed Intensive Inpatient Withdrawal Management): a more recent innovation, intended for persons with complex or even life-threatening symptoms. Hospital-based.
Some programs will provide multiple levels in the same facility or even on the same unit. That way a patient can stay in a familiar setting, with their current clinical team, and perhaps even avoid an unwelcome transfer to another service or institution.










{kind=link}